


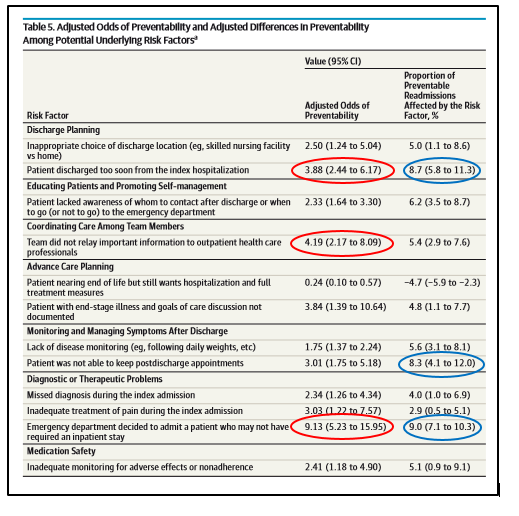
Love or hate readmission rates as an effective measure of institutional performance, the benchmark has become the coin of the realm for QI gurus, policy geeks, and stat crunchers. As such, we see new journal releases every week–mostly data dives into large registries where the conclusions proffered are tentative at best. Clinicians rarely get studies comprised of patient-level information whose findings may impact how to better organize their PI interventions and direct care. That just changed (see excerpted table at bottom).
Andrew Auerbach, MD MPH and colleagues just published, Preventability and Causes of Readmissions in a National Cohort of General Medicine Patients in JAMA IM, and the results merit a deeper look. Andy was kind enough to answer some questions regarding his group’s important paper for the blog.
 Q: Andy, first off, you and your collaborators should be congratulated on releasing the most exhaustive study on readmission root causes to date. For readers, can you tell us why your trial stands apart from the others and explain the findings?
Q: Andy, first off, you and your collaborators should be congratulated on releasing the most exhaustive study on readmission root causes to date. For readers, can you tell us why your trial stands apart from the others and explain the findings?
Auerbach: Thanks for the kind words – this was a gargantuan effort and involved nearly 100 people across all the HOMERuN sites – I’d run the risk of an Oscars acceptance speech if I tried to thank them all, but all of them have my deepest thanks.
Our study stands in contrast to others because we were truly national, and because we used a rigorous but reality-based review process to define preventability and its root causes. Our research also took the perspective that the patient or the illness was never the sole or even primary reason for readmission, and that if a readmission took place the system was to blame.
Q: You found a quarter of the patients in your cohort experienced a potentially preventable readmission. The number at first blush appears large. If one assumes a hypothetical readmit rate of say 16%, however, the universe of patients we might have an impact on lessens. Four percent. Through that lens, what can readers take away from your trial so they might improve the care of the remaining ninety-six?
Auerbach: I am not sure I agree with that view in terms of the readmitted patient group, but 4% – if applied across the hundreds of thousands of patients discharged each month – is still a very large absolute number of patients. Our study points out that preventable readmissions, whether prevalent in 4 or 8 or 12%, are still the minority of readmissions and need to be targeted with interventions in a prioritized manner which take into account the potential impact of each program.
Q: While we are on the four percent theme, what do you make of all the “exceptional” interventions of MCOs and hospitals these days—be it telehealth, home visits, or dedicated disease pathways? Not a month can go by most of us don’t hear or see some organization engaged in some self-promotion or chest-puffing touting their readmit rates reductions from greater than 20% to less than 10%. I worry about the message given the data you and others have produced. It matters because we need a real floor on how low we can drop the metric?
Auerbach: I agree that a readmission rate of zero or close to it is not reasonable, but I am quite unsure what the ‘right’ readmission rate is, because that number is a balance of patient preferences, societal preferences, and as you point out, payors’ needs. So as you are managing exceptional programs, or choosing them carefully, our research suggests that you should really focus on admitting patients carefully, carefully assessing readiness for discharge among higher risk patients, and creating a safe landing place in terms of self-care and home supports.
Q: You mention confounding and unmeasured variables in the discussion, perhaps limiting the analysis–as does the guest commenter. It’s a fact of life with this kind of research, though. So many things cluster together—and a myriad of patient experiences interconnect with multiplier effects we’ll never untangle. Do you think in the end, sussing out all the causes for return trips and the interventions to prevent them will lead us to the same place we started from? And by that I mean, a checklist of things we should apply to everyone and are on the clipboard already (medication reconciliation, set appointments, etc.)?
Auerbach: I think that interventions like BOOST, Naylor’s program, RED, etc. have taken a programmatic ‘checklist’ approach which is incredibly valuable, but which has not yet translated into a right-sized, patient-customized checklist approach which exists separately from these larger programs. There are indeed some mechanistic issues (discharge visits, medication reconciliation) which are important parts of the transition record, but our data suggest that cognitive issues around the ability to provide self-care or who to call after discharge are even more important. In many cases we reviewed, the documentation of discharge visits and call back numbers was quite clear, but patients were actually deeply unsure about how to use these resources.
Q: When I think of readmit rates and the CMS Hospital Readmissions Reduction Program (HRRP) these days, I am reminded of the old “less filling or taste great” saw. In the same vein, is the penalty reflecting an accurate quality measure or some utilization proxy hospitals have little control over? This is still unsettled science and the exchanges between the different camps while interesting to read, do not assist us in advancing where CMS will go with this measure or how we should apply it. What’s your opinion?
Auerbach: I think readmission is an important measure but a blunt tool for deciding on where/how to chip away at the complex pathophysiology of poor care transitions. Our data suggest that in many cases the readmission represents an error or problem which was produced by the acute care stay, but in an equally large proportion, the problems lay outside the hospital walls. The readmission measure, while applied to hospitals, is a cudgel to ensure that health systems create stronger primary care and post-acute systems. How to do that effectively is as yet unclear.
Q: Finally, perhaps you can add any other points of interest you might want readers to know about?
Auerbach: HOMERuN will continue to function, and we are looking for opportunities for sites to be our ‘V2’ wave of readmission adjudication and will be developing partnerships to support that work in the coming weeks. We are doing the usual range of secondary analyses on existing data as well, of course. The project will be an ongoing work in progress.
Of mention, co-released in the same issue: International Validity of the HOSPITAL Score to Predict 30-Day Potentially Avoidable Hospital Readmissions . (File under, can we build a better mousetrap?)
Leave A Comment