


Up for a 25% fee hit?
We approach January 1, and again the SGR cut looms heavy. However, now congress seeks to avert another patch with a long-term fix. Perhaps you have heard, but an actual bill might be in the works. While the final proposal has not seen daylight—a merged house and senate product needs tuning—the fee for service payment model we have grown comfortable with will undergo a rebirth. To earn greater or equal revenue, we will need to achieve prespecified process of care and health outcome targets (VBP or value-based payment) on top of the old reimbursement chassis. Additionally, participating in alternate payment models (APM’s), e.g., patient-centered medical homes, will garner increased rewards. A caveat, APM’s work for ambulists, but not for hospitalists—and SHM has responded to CMS with proposals. The same goes for VBP mismatches. Stay tuned.
Moreover, baseline annual fee for service updates for the next ten years would be flat, but we will have opportunities to earn greater payments within the above VBP design. Unfortunately, the proposal must be budget neutral, so some hospitalists will lose when others win.
Making the problem even harder to solve, to move on the fix, congress must purge a decade’s worth of SGR driven debt to eradicate the hole they dug for themselves. Postponing the solution cost us all a bucket load, $150B worth, so our legislators must search for “pay-fors” to offset the slate. Docs get the repair, but hospitals, device and drug companies, or post-acute facilities will be in the crosshairs to make the bill work. Below however, you will see irony.
A well-documented 2013 study from JAMA demonstrates contradiction. Despite the clamoring for change and new models of payment, (I did not say loss of revenue), make no mistake how tough the transformation will be. With all the chatter of, “we’re ready,” “pay for value,” and ” bring on integrated care,” recalcitrant docs are happy with the way things exist now, thank you very much.
See my red circle regarding our embrace for “liberating” FFS–7% worth–but do peruse the whole table: 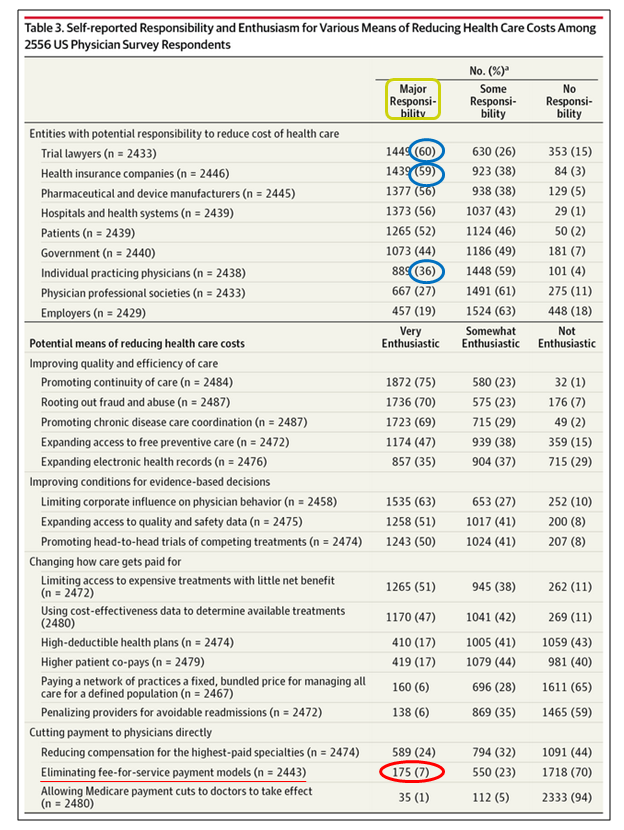 Well, if you like your FFS and RVUs, perhaps I can entice you with a new potential rub on our old friend. Instead of the usual RVU equation…:
Well, if you like your FFS and RVUs, perhaps I can entice you with a new potential rub on our old friend. Instead of the usual RVU equation…:
Total RVU = Work RVU + Practice Expense RVU + Malpractice Expense RVU
…now you can add the Value-based RVU:
Total RVU = Work RVU + Practice Expense RVU + Malpractice Expense RVU + Value-Based RVU:
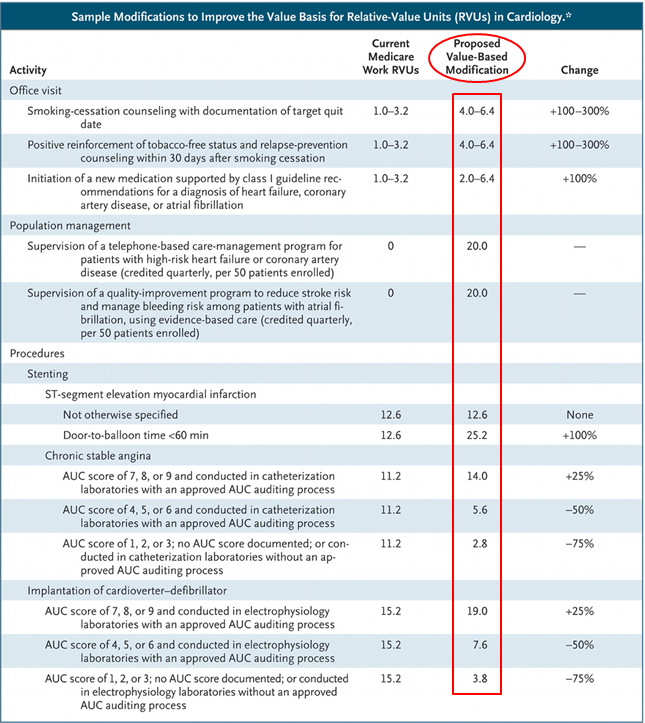
What a kludge-o-rama, and I don’t see any greater simplicity here beyond the P4P modifiers we already use or will implement. I could write a paragraph why, but will spare you the headache. Coming soon to a theater near you.
Our health system has the highest administrative costs in the world, bar none (slide #18). Look at your back office. The number of personnel needed to code and process our charts outnumbers us. The records and the methods we use to scrub them symbolize our cumbersome (and ? antiquated) FFS scheme. However, the same arrangement used to generate our bills, serves as the foundation to construct research projects, generate quality info, and synthesize RVU reports.
Do you see FFS and coding, with ICD-10 on the way, vanishing soon? Even with integrated care and payment bundling, we need the facts. The efforts required to make our next payment and QI prototype run, by default, will perpetuate current data collection methods, delaying its demise, and continue to prop up RVU/FFS as king. VBP and constructive payment add-ons will still serve as vassals.
How do some in the OECD perform the same coding tasks more efficiently and keep costs low. After all, no country has yet perfected or adopted natural language processing. I do not know, but I believe the U.S. will still need a sizable back office for at least another decade.
No way around things, we will be playing a new compensation ballgame, but with similar administrative burdens and costs.
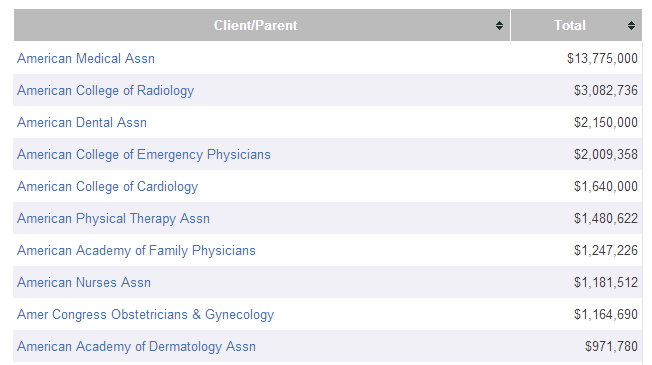
And if you have an interest regarding why we have the payment system we have, who among us might be more favored than others, and which organizations might be currying more favor with congress, you can read about the RUC or see below (2013 dollars spent on lobbying congress). That’s what the insiders call a high performance health system.
**On December 12th, the Senate Finance Committee will be holding an executive session and markup re: SGR repeal.***
UPDATE: It appears the Senate Finance and House Ways and Means committees released a more formed proposal on Dec. 4th. A short summary here, but most disturbing, we will likely see another 1-3 month patch to stave off the Jan 1 cut. Congress breaks for holiday recess on Dec 13th.
“Rep. Jim McDermott, top Democrat on the Ways and Means Health Subcommittee and a physician, said aides and lawmakers are “in turmoil” about how to approach SGR. Ultimately, he’s pessimistic about getting the formula repealed at all because of the disputes over how to pay for it.”
[…] Posted at The Hospital Leader on […]