


(Something I sent along to my PGYs. Thought you might enjoy. And think about where hospitalists fit into all of this)
A Porsche or a Prius?
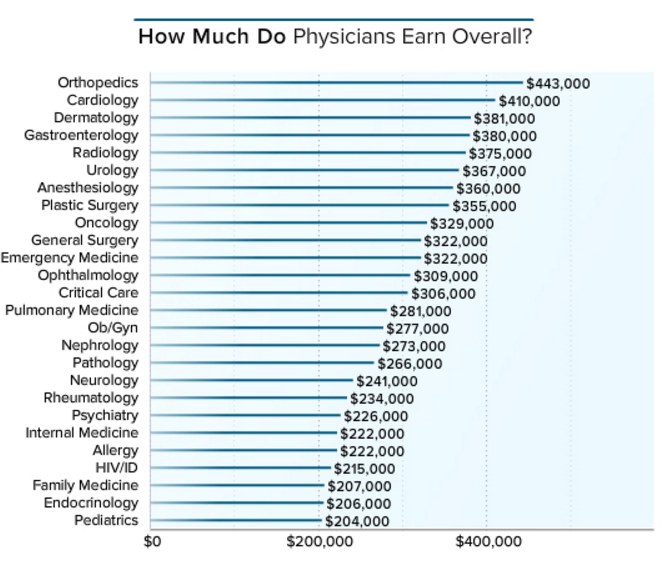
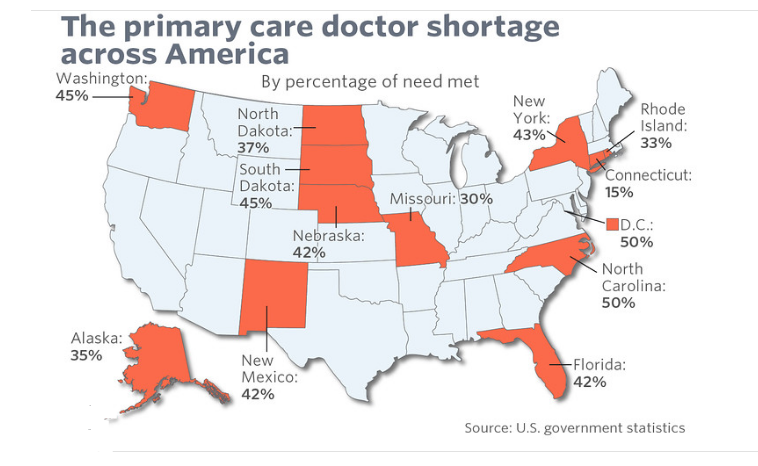
Have a look at the two figures below and see if you can spot the dilemma:
 See it? I knew that you could.
See it? I knew that you could.
Here’s the thing. We have lived with an arrangement that reimburses specialists more than generalists for greater than fifty years. You would think because that is so, the progenitors of the system knew what they were doing and assigned the right amount of compensation to each type of physician. Specialists and proceduralitsts do stuff so pay them more.
On one level, that makes sense. After all, you can see the results specialists achieve quickly given all those high tech thingies they use that come with instruction manuals. They produce big levels of patient satisfaction and often, get that instant cure. Folks liked that, and they ponied up for it. So much so that they drove the price tag up and up. As luck would have it, insurance companies–new on the scene back then–stepped up and helped pay those escalating bills. Good timing.
Conversely, old Doc Watson, the family provider, talked to you, nursed your sprained ankle, reassured your doubts about that lingering sore throat, and told you to stop after the second martini. You paid him a chicken or baked him a pecan pie. Insurance? We don’t need no stinking insurance.
Oversimplified, yes, but that train left the station and here we are a few decades later. Insurance companies, hospitals, and the government got captured by a powerful (and prosperous) contingent of specialty societies and the enterprise grew. Those bills kept getting paid.
Now we have an imbalance of specialty types, and it stems more from an accident of history than rational planning. That’s the substance of it. You might invoke years of training and sweat equity to justify loftier bucks. For some, that might apply (cardiothoracic, vascular and neurosurgery). However, tell that to all the psychiatrists, pediatric and medical cognitive specialists, and pathologists, to name a few. Nice theory. They are not exactly getting their just rewards.
Let me give you something to consider. If you flew down from Mars and had the opportunity to build our system anew–and knew nothing of prior entrenched attitudes and practices–how would you value each specialty? Better yet, if the zombie apocalypse was upon us, and there was one seat left on the bus to the promised land–and no physician was sitting in it–would you invite the electrophysiologist or the family practitioner to get on board? You need a physician, of course. The two of them are pressing their noses against the bus window clamoring for a seat after all. You have to make your choice. Gotta pick one.
So have a look at the table I mocked up below. The top row represents our current state of affairs. The remaining three rows below get at some other perspectives (HINT: umm, the bus was like a metaphor).
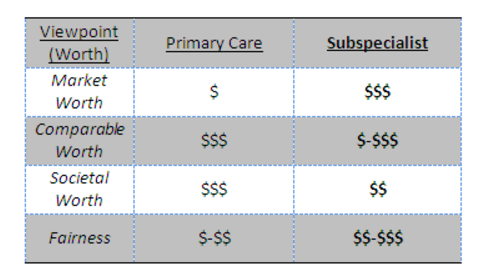
I suspect as the system tightens and baby step, incremental changes occur—you will see a shift and the paradigms of rows two to four will be brought to bear. Patients will shoulder more costs and have greater choice. So will Uncle Sam. The ship will not turn around in a decade, but I suspect in less than a generation, our healthcare system will have more parity. We are close to maxing the credit card. Primary care dollars will increase, or subspecialty dollars will come down. Or both. Something to ponder as you decide on your preferred path.
Reminds me of a joke…
Where do you hide a $5 bill from an anesthesiologist? Put in in the OR after 3 pm.
Where do you hide a $5 bill from a radiologist? Tape it to the patient.
Where do you hide a $5 bill from an orthopedist? Put it in a book.
Where do you hide a $5 bill from a surgeon? Tape it to his kid.
Where do you hide a $5 bill from a plastic surgeon? You can’t.
How do you hide money from a primary care physician?
Trick question. There isn’t any money in primary care.
One day we will surrender that joke.
Leave A Comment